That is interesting, but given with mouthwash you don’t drink it, you swish it and spit it out, so how much alcohol is getting into the bloodstream? It is a good question, it is why alcohol free mouthwashes exist.
I was thinking it was more the subjecting your mouth to contact with alcohol (in the mouthwash) that was potentially the problem. (For cancers of the mouth/tongue)
1 Like
With cancer they give base rates for each type of cancer, like x% will get breast cancer in their lifetime. Some people because of genetics have elevated risks for cancer, that would be above that base rate. That base rate itself varies between localities and countries, that can be attributable to genetics, but also may be influenced by things like air pollution or chemical pollution or things like smoking rates.
I don’t think anyone is saying if someone gets cancer it is their fault because they didn’t eat cleanly or whatever. You can do everything right and as the base cancer rate shows you can still get cancer.
1 Like
I could only stomach about 10 min of that Netflix documentary and then turned it off. Thought the guy was super weird and a little obsessed.
After some additional thought and introspection, I’ve decided that I really don’t care if people want to drink or not drink. It’s your life to live as you see fit. Just don’t be a butthead and put other people down who choose differently than you.
…which kind of applies to my philosophy pretty much all of my other views about other ‘big topics’ of discussion. ![]()
4 Likes
Personally, I have long since given up worrying much about what other people do with respect to impacting their health risk as long as it does not pose risk to others. (Ie. DUI and second hand smoke)
Yes, I know alcohol overuse, along with smoking, obesity and other factors are causes of increased health care costs for all of us. But I also see how much these habits can be ingrained and unlikely to change in many people.
In my work, I see patients at home for their health care. This week I went to see a patient just home from the hospital after pneumonia on top of her chronic pulmonary disease. She was complaining of the dust outside, poor air quality from the fires, even the neighbor’s cat relieving itself near her window all impacting her breathing. And I smell her cigarette smoke inside the house. Of course I will educate her on the health risk of continuing to smoke and at least make sure she is not smoking near her oxygen tanks, but she has heard all of this for decades.
3 Likes
I see you’ve read Outlive by Dr. Peter Attia!
To the rest of you in this thread, I highly recommend it. He doesn’t just have recommendations for how to live longer, but also how to live healthier.
1 Like
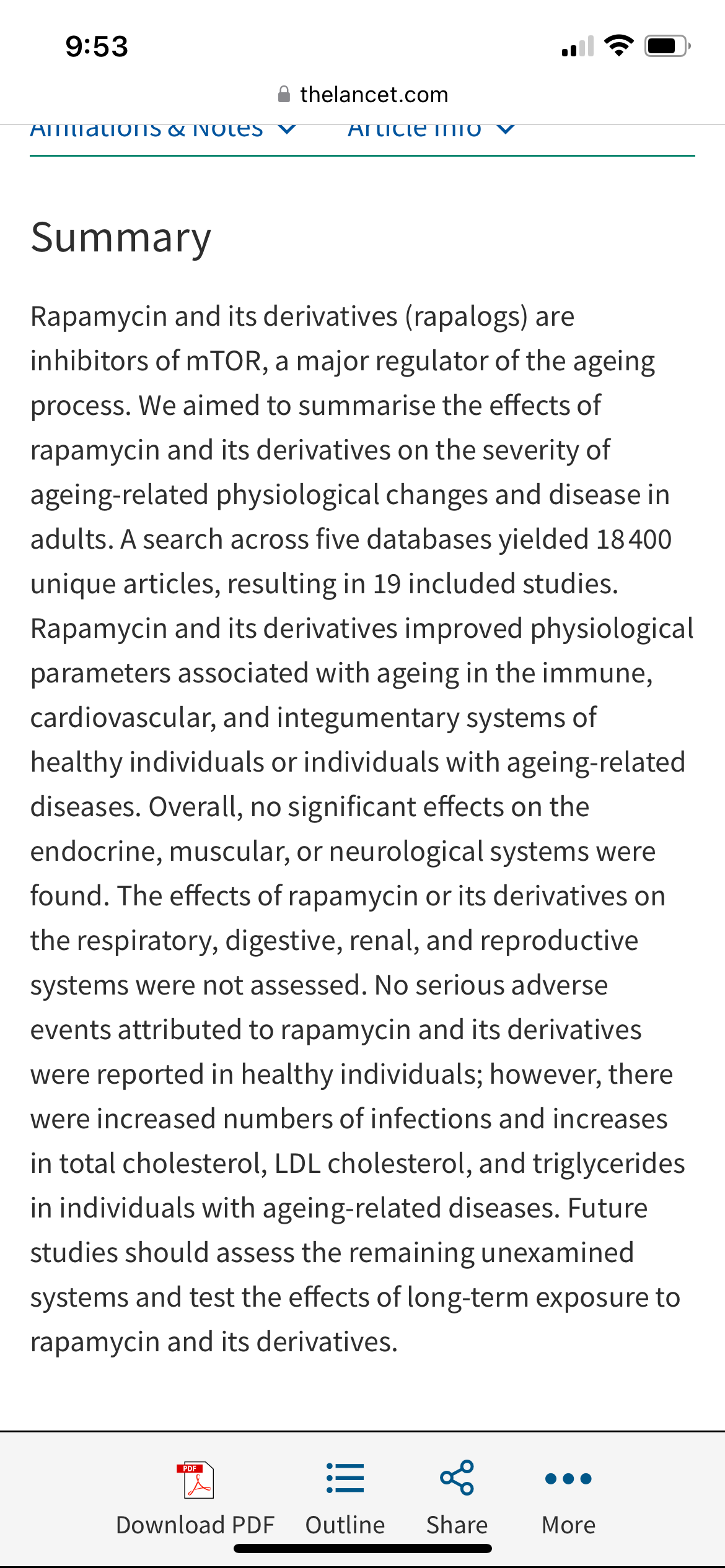
Take the recommendations in that book with a big grain of salt. He is a known peddler of rapamycin, an unproven “anti-aging” drug which should not be taken without a doctor’s guidance.
https://www.thelancet.com/journals/lanhl/article/PIIS2666-7568(23)00258-1/fulltext
Here is the abstract summarizing the findings:
4 Likes
Yes, I really enjoyed the book.
There are many excellent recommendations on sleep, nutrition, exercise, etc. And in terms of exercise, he writes about the “Four Pillars”, which are: stability. strength, aerobic efficiency and anaerobic performance.
He’s also a big believer in grip strength as one determiner of overall health and longevity.
And he’s a big believer “predictive healthcare”, such as DEXA scans.
1 Like
Yeah, I don’t like that he sells supplements, but that doesn’t mean he’s all wrong.
2 Likes
I don’t think he does sell supplements fyi.
Not directly, but he actively promotes questionable stuff. Wonder why?…
Anyhow, back to our regular discussion.
Thanks for the insight on Lp(a). Since Lp(a) is genetic and there doesn’t seem to much that can be done to lower it, I assume you are sharing the information about Lp(a) so that those with high Lp(a) can get proper preventative treatment and try to minimize other risk factors and reduce the risk of cardiovascular disease, for instance changing diet and exercise and even limiting alcohol consumption to control LDL.
I view information on the dangers of alcohol consumption similarly. For example, as I mentioned those with Afib (about 10 million Americans) ought to be aware that even moderate amounts of alcohol can be a trigger, leading to double the risk of an episode within 4 hours of the consumption of even one drink. Such information helps those with AFib choose whether drinking even moderate amounts of alcohol makes sense to them. Yet you characterize such information as dogmatic and misleading. I don’t get it?
To my mind, just as information about Lp(a) is worth sharing, so is information about the dangers of alcohol to those who have AFib, and higher risks of cancer, etc.
As for Lp(a), mine was checked by my cardiologist without my request, and was covered by insurance. If others doctors’ or cardiologists haven’t performed the test, request that they do. I see mine was only performed once which I assume is because it is genetic and doesn’t really change much.
1 Like
LDL needs to be lowered further than lifestyle changes will achieve. That typically means full dose statin, with possible addition of ezetemibe and a PCSK-9 inhibitor if those aren’t effective or tolerated.
2 Likes
This is a great summary. https://open.spotify.com/episode/1UVuQiniOMyRFGma7bC96z?si=SWDTLYJbRfSYG6P5H-SWcQ&t=1359&context=spotify%3Ashow%3A6SSr1fxyDOZSYhS7QeHJ4w
Gift link.
This article wouldn’t give a gift link so I’m not sure if you all can read it but it’s a fair summary (imo) of all the talk lately.
I just established care with a new internist yesterday. Her advice was very clear - stop drinking completely.
I am not overweight so I’ve never really been, “talked to,” about that. I’m getting the sense that people/docs in general have a lot easier time addressing alcohol consumption v food consumption. Obviously, the latter is more nuanced with a big distinguishing factor being no one needs alcohol, but we all need to eat.
No one likes to be scolded about anything, but I think alcohol is an easier one for docs to be hard-lined with than diet and exercise.
4 Likes
On the other hand its also even easier for people to lie to their doctor about how much they drink compared to how much they are dieting and exercising. For a start there’s less observable evidence compared to the visible impacts on your weight and fitness from success in dieting and/or exercising. So if a doctor scolds you about diet and exercise, they are clearly telling you that you’ve failed in that regard.
1 Like
The tide has really turned on docs talking to people about their weight, many docs won’t discuss weight with their patients unless asked…so no talk about losing weight, health risks, benefits of proper diet and exercise etc. Many offices aren’t even weighing people anymore for a number of reasons. Docs are caught between a rock and a hard place between doing their job and possibly making a patient feel uncomfortable, or being accused of fat shaming, blaming the patient, etc. NIDDK and other orgs give guidelines to docs and suggest first asking the patient if the doctor can talk with them about their weight and going from there. Docs definitely don’t want bad ratings on the various places patients can provide feedback.
I wonder how/if docs will continue to talk with patients about alcohol use considering what’s happening with overweight/obesity talk. Not sure how docs as a group see the alcohol/cancer risk data or if they will proactively bring it up with their patients. i will definitely ask my docs what they think when I see them next.
2 Likes